By: Dr. Virginia de la Lastra
I’d like you to meet Isabella. She is fifteen. It is summer — the most terrible time of the year.
On Tuesday, she goes to the mall with her friends to get waxed. When Isabella’s turn comes, the woman stops. She stares at her through thin linen curtains and says: “Why do you have so much hair? I’m going to have to charge you extra.” Her friends look at her. Isabella says nothing.
Three weeks ago, her mother took her to a dermatologist for her acne. He gave her creams. She asked about the hair. He said: “Oh, for that? You are a laser hair removal candidate.”
When she gets home, the hunger hits — hard, in sudden crashes she cannot explain. She is on a diet, and her mother is watching. So, Isabella eats in secret. Not a cookie. The whole package. Fast. In the dark. Standing up. Listening for footsteps.
Then the guilt comes. Because if she is hiding, she must be doing something wrong. She must be the problem. The nutritionist told her: “You just need to eat less. Go swimming!”
Her mother takes her to an endocrinologist. Surely this one will find what is wrong. He orders lab work but the results come back normal. He prescribes an oral contraceptive. The bleeding becomes regular and the acne begins to clear. The chart looks normal. Everyone moves on. But Isabella does not move on.
When symptoms are silenced instead of understood
Her weight increases. Her hunger crashes worsen. A sadness settles in permanently. She survives — because she tells herself this is what life must be like for everyone.
Seven years pass. Isabella is twenty-two. She walks into a different doctor’s office. And this doctor does something no one has done in seven years. This doctor does not manage. This doctor does not refer. She investigates. She orders tests no one has ordered before. She tests how Isabella’s body processes sugar. She measures a hormone no previous doctor had thought to check.
The results explain everything. Insulin resistance — an atypical form the standard tests had missed. Hormonal imbalance. Polycystic Ovary Syndrome (PCOS). Seven years of symptoms. One diagnosis. The treatment: metformin. Spironolactone. Simple. Affordable. Available in any pharmacy in the world.
In one year, Isabella loses thirty-four pounds. No extreme diet. No surgery. Her skin clears. The hair normalizes. She looks in the mirror and sees someone she has never met.
In medicine, we are taught that symptoms are clues. A fever tells you about infection. We do not treat a fever by turning off the thermometer. And yet — when it comes to women’s reproductive health, this is often done. A woman comes in with an irregular cycle, with pain, with mood changes. The question her doctor asks is: how do we restore a regular bleeding pattern? The answer, overwhelmingly, is hormonal intervention. The symptoms disappear. The chart looks normal. Everyone moves on.
But Isabella’s body was not malfunctioning. It was functioning perfectly — communicating exactly what was wrong. Her irregular cycle, her acne, the hair— these were not the problem. They were the message. And we silenced the messenger.
A system that normalizes instead of diagnoses
Each time Isabella left an office, she was symptomatically better and clinically worse. There is a certain kind of thinking that asks the wrong question. Not: is the tool suited to the problem? But: is the problem suited to the tool? Not: does the hat fit the head? But: how do we make the head fit the hat?
We turned the means into an end. A regular bleeding pattern and skin without acne became the goal — when it should have been a diagnostic tool. The question was never “how do we make her cycle look normal.” The question was “what is her cycle telling us about her health?”
When a healthcare system systematically fails to diagnose half the population because it treats their symptoms as inconveniences to be suppressed — this is not just a medical failure. This is a structural injustice.
So, how many Isabellas are there? How many of you have experienced irregular cycles, unexplained pain, fatigue, mood changes — and were told it was normal? How many of you were put on a pill and told the problem was solved? You may be Isabella.
What the data reveals
One in five women of reproductive age worldwide has PCOS. Not one in a hundred. One in five. And the prevalence is rising.
The sadness Isabella felt at sixteen was not a personality trait. It was not weakness. Research shows that 57% of women with PCOS have at least one psychiatric disorder — depression, anxiety, OCD. Her sadness had a name. It had a cause. And it was treatable. But no one connected it to what her body was trying to say.
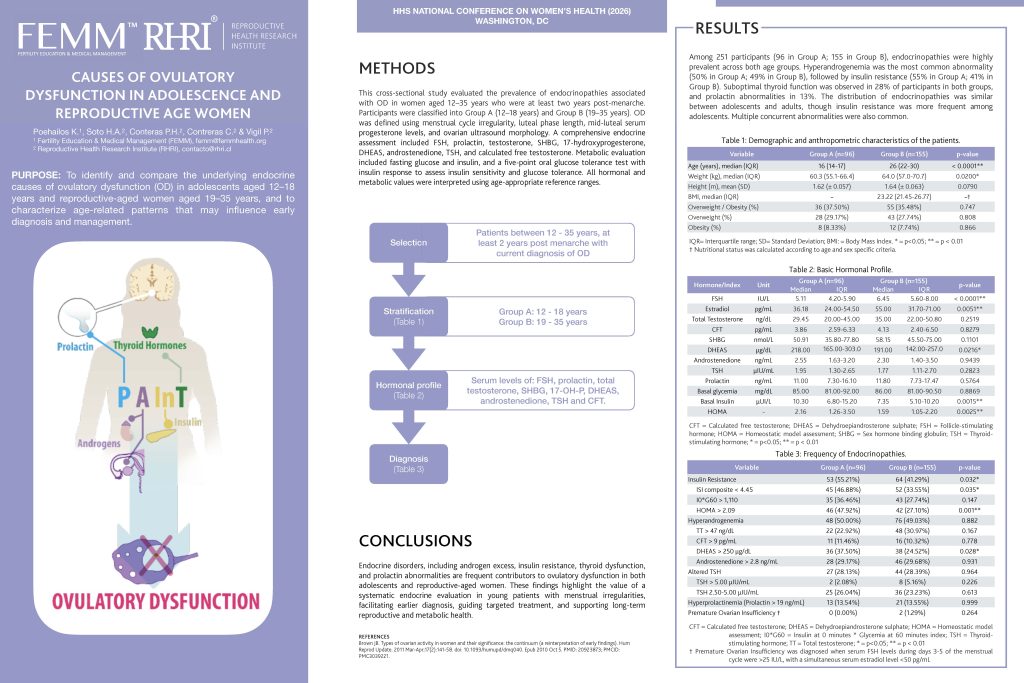
Last week in Washington, DC, we presented findings from 251 women and girls with menstrual irregularities. We ran a real investigation — not the standard panel, but the kind of comprehensive endocrine evaluation no one ran on Isabella for seven years. Twenty-six percent had sub-optimal thyroid function. Roughly half had hyperandrogenemia. More than half of the adolescents had insulin resistance. Not rare exceptions. The majority.
And here is what makes this devastating: the distribution was nearly identical between adolescents and adult women. What was not diagnosed at fifteen was still not diagnosed at twenty-five. The system failed them twice — at the same rate, a decade apart. That is hundreds of millions of women whose symptoms were silenced instead of interpreted.
And the failure doesn’t stop at diagnosis. Even when someone does listen — even when a woman finds a doctor who takes her seriously — there is a well-documented gap of seventeen years between what research discovers and when it reaches the average healthcare provider. Seventeen years. So even the women who are heard are being treated with tools that are almost two decades behind the science.
The cost of delayed diagnosis
We know that oral contraceptives — prescribed to an estimated 98% of adolescent girls with PCOS — produce a normal ovulation rate in only 12% of patients after treatment. The chart looked normal. The girl was not well. She was being channeled, quietly, toward the fertility crisis she would face a decade later. Isabella at fifteen was not just failed. She was set up to fail again at twenty-eight.
And the failure does not stop with her. The offspring of women with untreated PCOS carry more than double the risk of neuropsychiatric disorders. More than double. The consequences of not treating Isabella at fifteen do not end with Isabella. They move forward impacting her children, and the next generation.
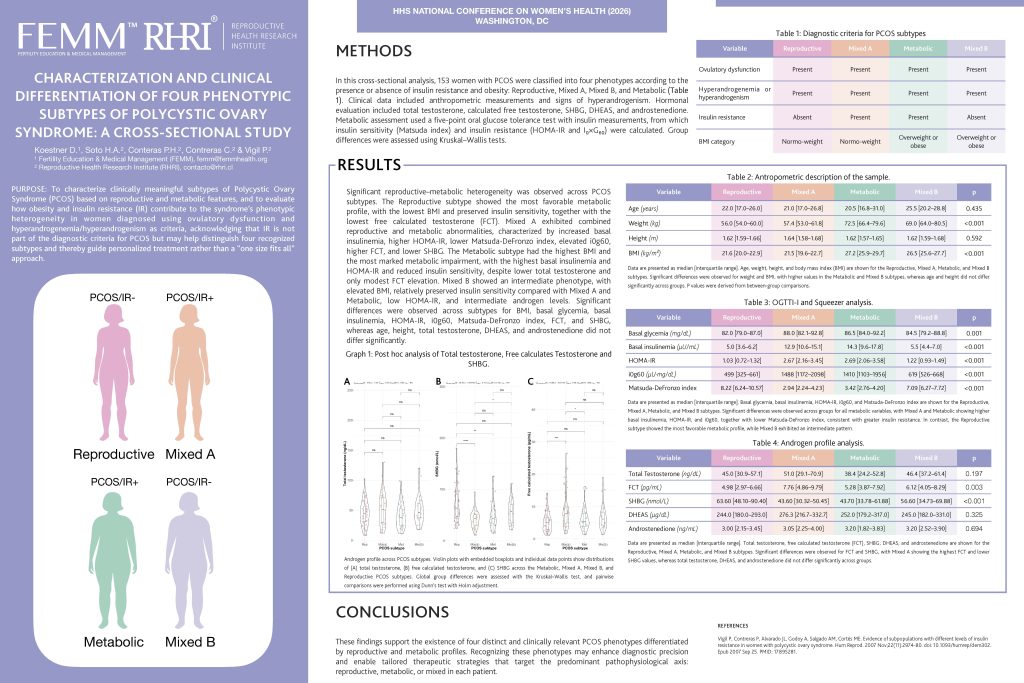
This is where our research becomes the bridge. We established that PCOS is not one condition — it has four distinct phenotypes, each requiring a different treatment approach. A one-size-fits-all protocol is not just ineffective. It is scientifically wrong.
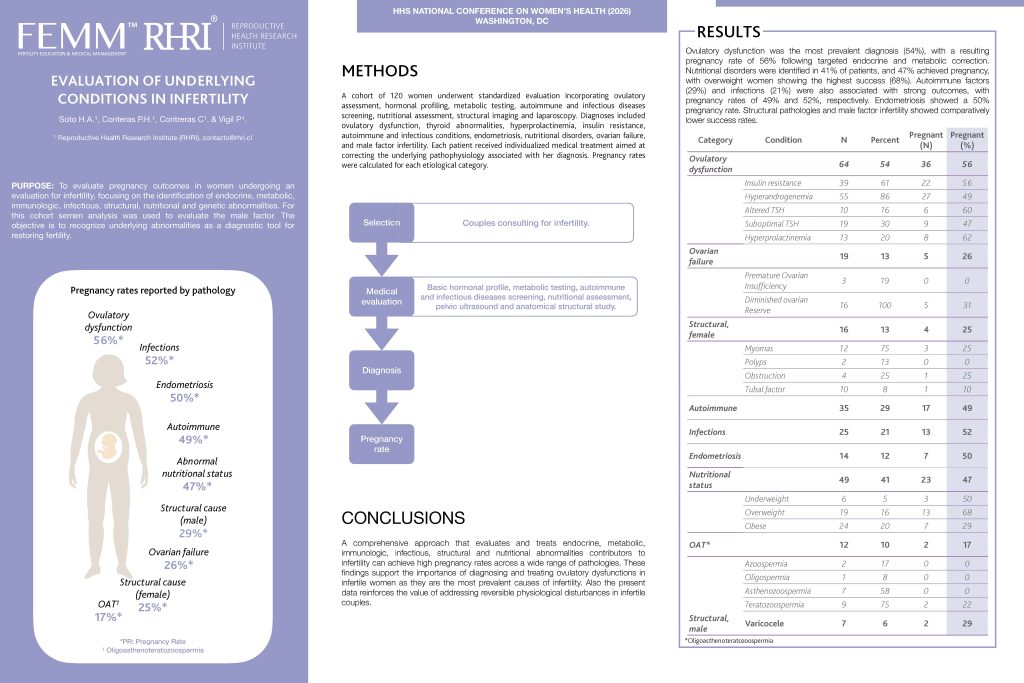
And we demonstrated that when you investigate instead of suppress — when you run the right tests and treat the underlying cause — more than half of women who were told they had a fertility problem conceive naturally. No surgery. No IVF. No new technology. Diagnosis and correction of what was already there, waiting to be read.
A better way forward
We shorten that seventeen-year gap. We don’t just want Isabella to be seen. We want her treated with the best, latest, evidence-based tools that exist. When we reversed the question — when we stopped suppressing and started listening — everything changed.
FEMM’s approach teaches women to read the signs their bodies are already producing. Cycle charting patterns. Biomarkers visible to any woman who knows what to look for. These are not problems to be managed. They are information to be understood. And when a woman understands that information, she becomes an active participant in her own healthcare — not a passive recipient of a prescription.
But knowledge alone is not enough. That knowledge must be connected to current, evidence-based medical support. This is what FEMM’s Medical Management program does: it trains doctors to diagnose and treat the underlying conditions, not just suppress the symptoms. It brings the latest research into the clinic.
And here is what makes this approach powerful: it works everywhere. The same knowledge, the same diagnostic tools, the same protocols — they work just as effectively in Manhattan as they do in a clinic in Nigeria or Tanzania.
Because once a woman has this knowledge, she carries it with her. It does not run out. It does not depend on a supply chain. And it requires only basic laboratory settings that already exist in most healthcare systems around the world.
This is not a program for privileged women. This is healthcare that meets women where they are — in high-resource and low-resource settings alike. Accessible. Affordable. Grounded in the best science we have.
Isabella is thriving today. After fifteen years of being told she was the problem — after learning, finally, to read herself — she is now teaching other women to do the same.
The real injustice is not just misdiagnosis. It is that millions of women were never taught to read their own bodies. Left illiterate about themselves — and therefore powerless. The system did not just fail to diagnose them. It failed to give them the language to even ask the right question.
The knowledge exists. The protocols exist. The bridge exists — and we are crossing it, every day, one woman at a time.